

Introduction:
The risk of venous thromboembolism (VTE) is increased in patients with cancer and contributes to significant morbidity, treatment delays and mortality. The Khorana score is the most well-validated VTE risk prediction tool that guides use of prophylactic anticoagulation in patients with cancer. The Khorana score includes cancer type, body mass index (BMI), hemoglobin, platelet count and leukocyte count but not a prior history of VTE which may increase the risk of recurrent VTE. Scant published data have suggested that a personal history of VTE increases the risk of VTE recurrence by 2 to 7-fold after cancer diagnosis. In this study, we examine the impact of history of VTE on VTE recurrence in a large cohort of patients with cancer.
Methods:
We performed a retrospective cohort study of patients diagnosed with cancer using aggregated de-identified data from electronic medical record of >300 major hospitals in US (IBM Watson Explorys). Patients with a personal history of VTE (deep vein thrombosis and/ or pulmonary embolism) more than one year prior to the diagnosis of cancer were included. Within this cohort, patients who developed recurrent VTE within 180 days of diagnosis of cancer were identified. The primary end-point was the incidence of cancer associated VTE (CVTE) in patients with prior history of VTE as compared to patients without history of VTE. Baseline characteristics including age, race, gender, BMI, prothrombotic mutations (Factor V Leiden, prothrombin gene 20210A mutation), antineoplastic agent use, cancer type and laboratory values (as included in Khorana risk score) were compared in all patients.
Results:
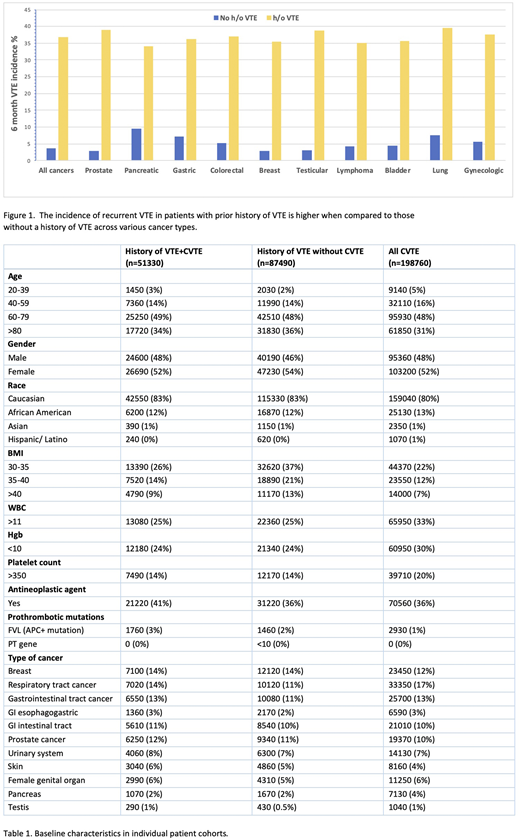
A total of 4,159,400 patients with a diagnosis of cancer were included. Of these, 138,820 patients (3.3%) had a history of VTE >1 year prior to being diagnosed with cancer. The incidence of CVTE at 180 days was 10-fold higher in those with prior history of VTE compared to those without (36.9% vs 3.66%; OR 15.4, 95% CI 15.22-15.6, P value <0.0001). While the inherent risk of CVTE varied based on cancer type (highest risk of 10.5% in pancreatic cancer), the risk of recurrent VTE in patients with prior VTE history is magnified to a similar degree across all cancer types as shown in Figure 1. Baseline characteristics including age, race, gender and cancer type distribution were similar in all groups, as shown in Table 1. Factor V Leiden mutation or activated protein C resistance (FVL/APC) was more prevalent in patients with prior history of VTE and subsequent CVTE (3%) as compared to all patients with CVTE regardless of history (1%), as shown in Table 1. A higher BMI was noted in patients with prior history of VTE (49% and 71% respectively in patients with and without CVTE) as compared to 41% in all patients with CVTE. Greater use of antineoplastic agents (41%) was noted in the group of patients with prior history of VTE and subsequent CVTE as compared to patients with prior VTE but no CVTE (36%).
Conclusion:
Our study highlights that a prior personal history of VTE >1 year before cancer diagnosis significantly increases the risk of cancer associated VTE independently, regardless of other established risk factors for VTE suggesting that this group of patients, especially those undergoing anti-cancer treatment may benefit from prophylactic anticoagulation. Increased incidence of FVL/ APC in patients with prior history of VTE and recurrent CVTE may reflect increased testing for prothrombotic mutations in this cohort. Our ongoing efforts include examining the effect of addition of history of VTE to the Khorana score. Finally, large prospective observational studies would be key to assess the impact of history of VTE on cancer thrombosis.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal